准分子激光治疗复杂冠脉病变的最新综述(上)|安贞心语2020盘点系列

准分子激光斑块消蚀术(ELCA)在经皮冠状动脉介入治疗(PCI)中的应用已有二十多年的历史。早期的经验看ELCA并不比单纯球囊的血管成形术有利;但随着操作技术的改进和适宜患者的选择,ELCA作为一种安全有效的动脉粥样硬化消蚀策略,已经在当代PCI中确立了自己的市场地位。随着世界范围内复杂冠状动脉介入治疗经验的增加,ELCA已成为动脉粥样硬化治疗的重要工具之一,与其他动脉粥样硬化治疗手段相比具有独特的优势。
目前ELCA通常用于支架内再狭窄、支架扩张不良、球囊不能通过的病变和慢性完全闭塞的患者。在过去25年中,在大多数情况下ELCA技术成功率>80%,血管夹层和穿孔等并发症的发生率平均为9%。在这篇综述中,我们对ELCA系统、其在当代PCI时代的实际应用、适应证和操作技术进行了全面系统的综述。
作者:韩伟 刘巍 首都医科大学附属北京安贞医院
内容简介
基础篇(上篇):
1.引言
2.文献回顾
3.准分子激光作用机制
4.操作人员控制
5.适应证
技术篇(下篇):
6.推荐的技术
7.导管特性
8.消蚀范围
9.激光成功的定义
10.安全性/并发症
11.血管内成像指导
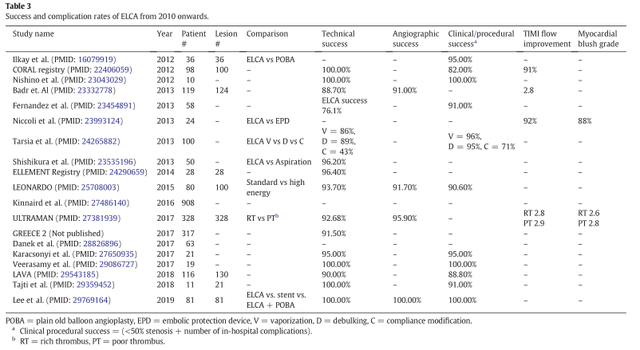
12.现代ELCA文献汇总及未来方向
13.结论
01
引言
自1992年以来,应用准分子激光(受激辐射分子光放大,LASER)进行冠状动脉介入治疗一直在美国使用。早期用于外周介入[1],随后是冠状动脉介入[2-5]。早期的ELCA伴随着严重的并发症,如靶血管夹层和穿孔。随着操作经验、患者选择和技术迭代的改善,由于能够提供更高的能量和更低的产热率,并发症发生率已显著降低。可获得更大范围导管尺寸以及器械通过性能的提高,促进了ELCA在各种PCI治疗中的采用。
目前美国唯一可用的冠状动脉准分子激光系统是第二代冷激光系统(CVX-300),由Spectrantics制造。随着越来越多的复杂冠状动脉介入治疗[6],ELCA已成为斑块修饰的关键工具。据报道,在2010-2019年期间,大约使用了5万个ELCA导管。ELCA虽然不像其他专用的斑块切除器械可对致密的钙化进行修饰,但它在治疗支架内再狭窄(ISR)和慢性完全闭塞(CTO)等复杂的冠状动脉介入治疗中有其独特的优势[7]。在复杂冠状动脉介入治疗的复兴的背景下,我们对ELCA系统、其在当代PCI时代的实际应用、适应证和操作技术进行了全面系统的回顾。
02 文献回顾
我们通过遵循系统综述和荟萃分析(PRISMA)检查表的首选报告项目进行了系统的文献搜索[8]。我们使用MEDLINE、EMBASE和CochraneLibrary进行了计算机检索至2019年8月16日。使用以下关键词:“激光”和冠状动脉(”coronary”OR“coronary artery” OR “coronaryvessel”)和(“动脉粥样硬化”或“经皮动脉粥样硬化”或“腔内动脉粥样硬化切除术”)。关键词:“LASER”AND(“冠状动脉”或“冠状动脉”或“冠状动脉血管”)AND(“经皮腔内斑块旋切术”或“经皮动脉粥样硬化切除术”或“腔内动脉粥样硬化切除术”)。
我们根据标题和摘要手动筛选参考文献列表,并纳入报告ELCA的适应证、成功率或并发症的前瞻性队列和病例对照研究。然后对全文的合格性进行了评估。我们的研究仅限于对人体研究。以非英语发表的病例报告和论文被排除在外(图1)。
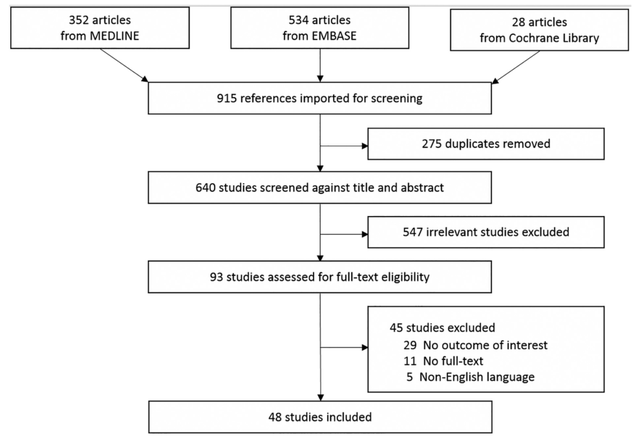
图1. 流程图显示了根据系统评审和荟萃分析(PRISMA)检查表的首选报告项进行系统搜索的步骤。47项研究纳入我们的综述。
03 准分子激光作用机制
ECLA采用氯化氙单色光激发激光器,产生波长为308nm的紫外光脉冲,脉冲频率25~80Hz,能量密度30~80mJ/mm,穿透深度<10~50μm。每一次脉冲,光都会被吸收。光很容易被斑块和血栓以相似的方式吸收[9]。光能吸收几乎瞬间释放出激光诱导的压力波。压力波引发快速的流体置换,从而导致汽泡的形成和坍塌。这会导致斑块的蒸发和清除。这种斑块改良可以通过球囊血管成形术病变准备实现更好的管腔扩张。有三种主要的作用机制(图2):
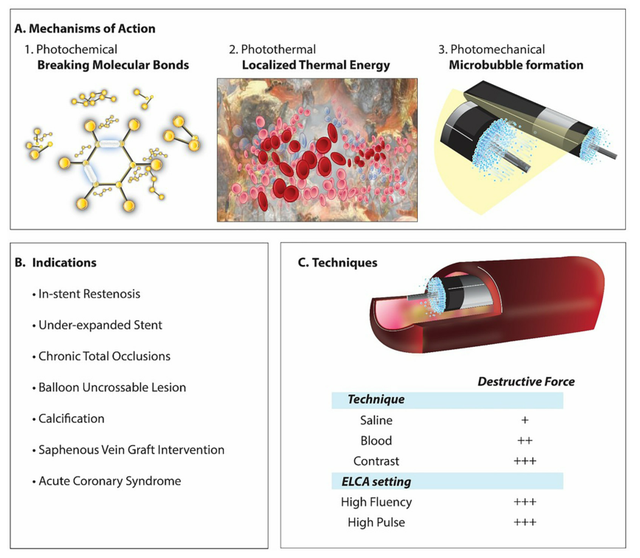
图2. 准分子激光导管动脉粥样硬化切除术(A)的三种主要作用机制协同作用,为ELCA提供了动脉粥样硬化斑块修饰的作用。在现代复杂冠状动脉介入治疗时代,最常用的适应证是钙化、ISR、支架扩张不良、球囊不能通过病变和CTO病变(B)。操作员需要熟悉ELCA设置以及不同的推送液体的方法,以提供更强的破坏力(C)。
(1)光化学反应
308nm光子的能量大于某些分子键的结合能。这会导致分子解离,导致机械键断裂[10,11]。
(2)光热效应
光子被血流中细胞的大分子吸收。这种振动导致产热率更高超过水的蒸发温度,并最终爆炸形成气相[12]。产生的热能导致动脉粥样硬化内胶原和蛋白质纤维的软化。
(3)光力学作用
气泡的快速膨胀和内爆导致导管尖端前方斑块的声学-力学破坏,且穿透较浅[13,14]。这被认为是ELCA将目标成分分解成小颗粒的主要机制[15]。
04 操作人员控制
目前可用的准分子激光系统如图3所示。ELCA导管在送入病变前需要校准。这是通过将导管尖端指向CVX-300主体上的校准端口来实现的。应谨慎行事,以确保无菌状态。一旦选择了导管并进行了校准,就可以调整通量(Fluence)和脉冲速率。通量控制气泡的大小,脉冲速率控制气泡的膨胀和收缩[16]。增加这些设置会导致更大的斑块破裂和管腔增加,但也会增加血管夹层和穿孔等并发症的风险。
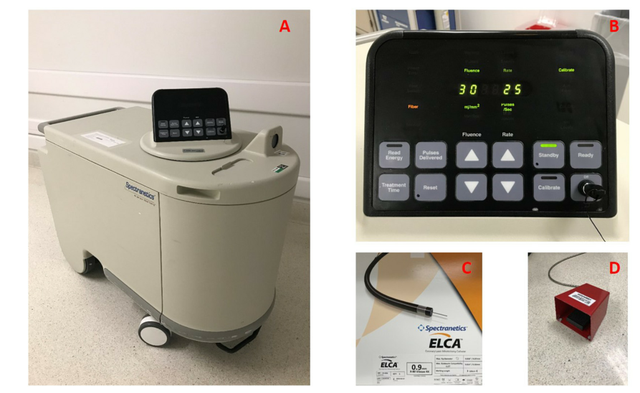
图3. CVX-300系统被 (A)。接通电源,进行5分钟的预热,完成后,应用自带的校准导管进行校准。然后,用选择的导管尺寸校准设备,确保导管尖端靠近校准端口的中心。校准后,能量和脉率将根据操作员的习惯进行调整(B)。将导管放入病变部位(C),助手按下控制面板上的READY按钮,并按下脚踏板以激活ELCA(D)。
(1)导管大小选择
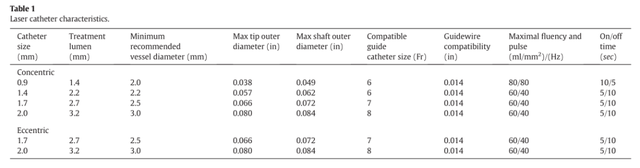
导管大小的选择对ELCA的成功起着至关重要的作用。它不仅决定了ELCA导管的输送性能,而且还决定了最大能量和脉冲重复频率,从而决定了有效的治疗范围(表1)。导管的特性将在本文后面介绍。
(2)通量(Fluence)
紫外光穿透组织并产生蒸汽所需的阈值能量称为通量[17]。
CVX-300激光发射器的范围在30到80mJ/mm2之间[18]。光能量越高,提供给病变的光机械效果就越多。能量越低,光化学效应越小。
(3)脉冲重复频率
在一秒周期内发射的脉冲数是脉冲重复率或频率,可在25至80 Hz之间调节[18]。脉冲重复次数越高,破坏力越大。CVX-300具有基于重复频率的标准脉冲宽度。使用说明(IFU)建议操作员开始时应根据感兴趣的病变量身定做较低的能量和速率。IFU中没有推荐的特定设置。
05 适应证
总体目标是使支架更容易输送,增加支架扩张,并避免无复流或远端栓塞等问题[13,14,16,19]。以下是ELCA辅助PCI的可接受适应证列表(图2,表2):

(1)支架扩张不良
在支架扩张不良的情况下,ELCA可以在不破坏支架结构[17,20,21]的情况下修饰潜在的顽固性动脉粥样硬化[17,20,21],随后改进支架扩张情况[22,23],从而降低支架内血栓形成的风险,改善支架的内皮化。这种效果可以通过最大限度地增加能量和脉冲频率,“座”在病灶上,以及在激光脉冲期间使用对比剂注射来优化[22-26]。
(2)支架内再狭窄(ISR)
与支架扩张时的目标类似,ELCA能够使现有支架进一步扩张,有助于减少斑块负担、修饰支架下的斑块和扩大血管管腔。在这种情况下,ELCA的成功率从91%提高到100%[19,27-29];与IVUS和OCT评估的单独球囊血管成形术相比,ELCA的横截面积和管腔增益更大[27]。OCT成像显示,在治疗再狭窄段时,ELCA同时消融管腔和腔外动脉粥样硬化成分[17,29,30]。因此,如果再狭窄的机制部分是支架扩张不良,ELCA增加了实现更大的支架扩张和更持久的长期结果的可能性[17]。
如果ELCA术后残余直径<30%,ISR复发率和主要不良心血管事件发生率较低[28,31]。因此,支架内组织的斑块消蚀是ELCA术后取得良好临床过程的关键。
然而,在ISR患者中,很少或没有随机数据将激光与其他动脉粥样硬化设备(如旋磨术、血管内碎石术)或与IVUS指导的球囊扩张(有或没有药物涂层)进行比较。虽然ELCA的潜在好处是去除分叉脊部的斑块、降低侧支阻塞的风险、避免复杂支架植入和其他装置斑块切除装置[17],但也有用于分叉病变时导致夹层和穿孔的报道[32]。与任何动脉粥样硬化切除装置一样,应避免在成角较陡的分叉病变使用ELCA[32-34],除非是极少数情况,如治疗ISR。
(3)钙化
重度钙化病变通常需要动脉粥样硬化切除才能成功地输送支架,达到最佳扩张。有多种器械可以增加支架扩张,如旋磨动脉粥样硬化切除术、血管内碎石术和ELCA。
ELCA可以破坏钙质结构,从而改善球囊扩张和支架扩张[7,18,24,32,34-41]。虽然ELCA用于钙化病变可能不是原发血管病变的第一选择,但在已经存在的支架后有大量钙化的情况下,激光在改变钙质结构方面比其他设备有独特的优势。
Lee等人报道称,在23名支架扩张不足导致ISR后的钙化病变接受ELCA治疗的患者中,通过光学相干断层扫描(OCT)评估,使用ECLA与更多的钙质断裂(61% vs 12%,单纯球囊血管成形术为12%)相关[42]。与那些单纯接受球囊血管成形术的人相比,ELCA能明显增加最小支架面积(6.15mm2 vs 4.65mm2)。
(4)球囊无法通过的病变和CTO
ELCA可软化硬斑块,允许器械通过CTO病变而无需更换导丝。ELCA在导丝通过病变但无法通过球囊或微导管以便更换介入导丝的情况下最有用。此外,ELCA后可以和冠脉旋磨术共同应用[43]。据报道,在CTO病例中,ELCA的成功率为86-100%[43-46]。
从技术角度来看,对于CTO病例,通常不在激光-病变界面使用生理盐水,因为通常要避免顺行注射,以防扩大夹层范围。此外,盐水不太可能到达激光-组织界面[17]。但是,重要的是要记住,长时间的激光脉冲可能会导致金属丝涂层的破坏和涂层粘在导管上[16]。
(5)其他
据报道,ELCA可以汽化血栓[47],降低远端栓塞的风险[48],清除潜在的斑块,并抑制血小板聚集[49]。ELCA还存在“血小板顿抑”现象,紫外光和血小板之间的相互作用会导致聚集动力学改变,进而导致血小板聚集减少和血小板聚集力的减弱[50]。
虽然ELCA在血栓负荷较高的大血栓血管中的应用已有报道,但目前尚无随机数据将激光与血栓抽吸术或针对冠脉血栓的更积极的药物治疗进行比较,因此,激光在ACS中的作用尚不清楚。
ELCA过去在移植静脉介入中已有报道。移植静脉介入存在固有的斑块和血栓栓塞风险[50-52]。ELCA可以汽化血栓,清除新生内膜增生,从而降低远端栓塞的风险。
鉴于近年来CTO的不断进展,随着操作人员选择治疗闭塞的原位血管,SVG-PCI的频率可能会降低。尽管如此,当必须行SVG-PCI时,ELCA被认为是一种少见、但必要的、应慎重应用的辅助治疗工具。ELCA的成功率在82%到97%之间,与其他适应证相比,远期的并发症发生率更高,从1%到7.5%不等[50,53-55]。
参考文献
[1] ChoyDS. History of lasers in medicine. Thorac Cardiovasc Surg. 1988;36(Suppl.2):114-7.
[2] CookSL, Eigler NL, Shefer A, Goldenberg T, Forrester JS, Litvack F. Percutaneous excimerlaser coronary angioplasty of lesions not ideal for balloon angioplasty.Circulation. 1991;84:632-43.
[3] KosterR, Kahler J, Brockhoff C, Munzel T, Meinertz T. Laser coronary angioplasty: history,present and future. Am J Cardiovasc Drugs. 2002;2:197-207.
[4] BittlJA, Sanborn TA, Tcheng JE, Siegel RM, Ellis SG. Clinical success, complicationsand restenosis rates with excimer laser coronary angioplasty. The Percutaneous ExcimerLaser Coronary Angioplasty Registry. Am J Cardiol. 1992;70:1533-9.
[5]Geschwind HJ, Dubois-Rande JL, Zelinsky R, Morelle JF, Boussignac G.Percutaneous coronary mid-infra-red laser angioplasty. Am Heart J. 1991;122:552-8.
[6] KirtaneAJ, Doshi D, Leon MB, et al. Treatment of higher-risk patients with anindication for revascularization: evolution within the field of contemporarypercutaneous coronary intervention. Circulation. 2016;134:422-31.
[7] KaracsonyiJ, Armstrong EJ, Truong HTD, et al. Contemporary use of laser duringpercutaneous coronary interventions: insights from the laser veterans affairs(LAVA) multicenter registry. J Invasive Cardiol. 2018;30:195-201.
[8] MoherD, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviewsand meta-analyses: the PRISMA statement. Int J Surg. 2010;8:336-41.
[9] EstellaP, Ryan Jr TJ, Landzberg JS, Bittl JA. Excimer laser-assisted coronaryangioplasty for lesions containing thrombus. J Am Coll Cardiol. 1993;21:1550-6.
[10]Litvack F, Grundfest WS, Goldenberg T, et al. Pulsed laser angioplasty:wavelength power and energy dependencies relevant to clinical application.Lasers Surg Med. 1988;8:60-5.
[11]Nakabayashi K, Sunaga D, Kaneko N, et al. Simple percutaneous coronaryinterventions using the modification of complex coronary lesion with excimerlaser. Cardiovasc Revasc Med. 2019;20:293-302.
[12] vanLeeuwen TG, Meertens JH, Velema E, Post MJ, Borst C. Intraluminal vapor bubble inducedby excimer laser pulse causes microsecond arterial dilation and invaginationleading to extensive wall damage in the rabbit. Circulation. 1993;87:1258-63.
[13]Biamino G. The excimer laser: science fiction fantasy or practical tool? JEndovasc Ther. 2004;11(Suppl. 2):II207-22.
[14] TopazO. A new, safer lasing technique for laser-facilitated coronary angioplasty. J IntervCardiol. 1993;6:297-306.
[15]Esenaliev RO, Oraevsky AA, Letokhov VS, Karabutov AA, Malinsky TV. Studies of acousticaland shock waves in the pulsed laser ablation of biotissue. Lasers Surg Med.1993;13:470-84.
[16]Coronary Atherectomy and Transradial Access Part I of III: Laser Atherectomy.2016. (Accessed 11/27/18, 2018, at https://www.cathlabdigest.com/article/Coronary-Atherectomy-Transradial-Access-Part-I-III-Laser-Atherectomy.)
[17]Rawlins J, Din JN, Talwar S, O’Kane P. Coronary intervention with the excimer laser: review of thetechnology and outcome data. Interv Cardiol. 2016;11:27-32.
[18] BadrS, Ben-Dor I, Dvir D, et al. The state of the excimer laser for coronaryintervention in the drug-eluting stent era. Cardiovasc Revasc Med. 2013;14:93-8.
[19] TchengJE, Wells LD, Phillips HR, Deckelbaum LI, Golobic RA. Development of a new techniquefor reducing pressure pulse generation during 308-nm excimer laser coronaryangioplasty. Cathet Cardiovasc Diagn. 1995;34:15-22.
[20]Papaioannou T, Yadegar D, Vari S, Shehada R, Grundfest WS. Excimer laser (308nm) recanalisation of in-stent restenosis: thermal considerations. Lasers MedSci. 2001; 16:90-100.
[21] BurrisN, Lippincott RA, Elfe A, Tcheng JE, O’Shea JC, Reiser C.Effects of 308 nanometer excimer laser energy on 316 L stainless-steel stents:implications for laser atherectomy of in-stent restenosis. J Invasive Cardiol.2000;12:555-9.
[22] SunewJ, Chandwaney RH, Stein DW, Meyers S, Davidson CJ. Excimer laser facilitated percutaneouscoronary intervention of a nondilatable coronary stent. Catheterization andCardiovascular Interventions: Official Journal of the Society for CardiacAngiography & Interventions. 2001;53:513-7 [discussion 8].
[23] LamSC, Bertog S, Sievert H. Excimer laser in management of under expansion of a newlydeployed coronary stent. Catheterization and Cardiovascular Interventions: OfficialJournal of the Society for Cardiac Angiography & Interventions. 2014;83: E64-8.
[24] LatibA, Takagi K, Chizzola G, et al. Excimer Laser Lesion modification to expandnondilatable stents: the ELLEMENT registry. Cardiovasc Revasc Med. 2014;15:8-12.
[25]Karacsonyi J, Danek BA, Karatasakis A, Ungi I, Banerjee S, Brilakis ES. Lasercoronary atherectomy during contrast injection for treating an underexpandedstent. JACC Cardiovasc Interv. 2016;9:e147-8.
[26] EgredM. A novel approach for under-expanded stent: excimer laser in contrast medium.J Invasive Cardiol. 2012;24:E161-3.
[27] MehranR, Mintz GS, Satler LF, et al. Treatment of in-stent restenosis with excimer lasercoronary angioplasty: mechanisms and results compared with PTCA alone.Circulation. 1997;96:2183-9.
[28] DahmJB, Kuon E, Vogelgesang D, et al. Relation of degree of laser debulking ofinstent restenosis as a predictor of restenosis rate. Am J Cardiol. 2002;90:68-70.
[29]Nishino M, Lee Y, Nakamura D, et al. Differences in optical coherencetomographic findings and clinical outcomes between excimer laser and cuttingballoon angioplasty for focal in-stent restenosis lesions. J Invasive Cardiol.2012;24:478-83.
[30]Rawlins J, Talwar S, Green M, O’Kane P. Optical coherence tomography following percutaneouscoronary intervention with excimer laser coronary atherectomy. CardiovascRevasc Med. 2014;15:29-34.
[31] DahmJB. Excimer laser coronary angioplasty (ELCA) for diffuse in-stent restenosis: beneficiallong-term results after sufficient debulking with a lesion-specific approachusing various laser catheters. Lasers Med Sci. 2001;16:84-9.
[32]Nishino M, Mori N, Takiuchi S, et al. Indications and outcomes of excimer lasercoronary atherectomy: efficacy and safety for thrombotic lesions-the ULTRAMANregistry. J Cardiol. 2017;69:314-9.
[33]Shishikura D, Otsuji S, Takiuchi S, et al. Vaporizing thrombus with excimerlaser before coronary stenting improves myocardial reperfusion in acutecoronary syndrome. Circ J. 2013;77:1445-52.
[34]Ambrosini V, Sorropago G, Laurenzano E, et al. Early outcome of high energylaser (excimer) facilitated coronary angioplasty ON hARD and complex calcifiedand balloon-resistant coronary lesions: LEONARDO study. Cardiovasc Revasc Med. 2015;16:141-6.
[35] BaimDS, Kent KM, King 3rd SB, et al. Evaluating new devices. Acute (in-hospital)results from the new approaches to coronary intervention registry. Circulation.1994;89:471-81.
[36]Baumbach A, Bittl JA, Fleck E, et al. Acute complications of excimer lasercoronary angioplasty: a detailed analysis of multicenter results.Coinvestigators of the U.S. and European Percutaneous Excimer Laser CoronaryAngioplasty (PELCA) registries. J Am Coll Cardiol. 1994;23:1305-13.
[37] SafianRD, Freed M, Reddy V, et al. Do excimer laser angioplasty and rotationalatherectomy facilitate balloon angioplasty? Implications for lesion-specificcoronary intervention. J Am Coll Cardiol. 1996;27:552-9.
[38]Reifart N, Vandormael M, Krajcar M, et al. Randomized comparison of angioplastyof omplex coronary lesions at a singlecenter. Excimer Laser, Rotational Atherectomy, and Balloon AngioplastyComparison (ERBAC) study. Circulation. 1997;96:91-8.
[39] GiriS, Ito S, Lansky AJ, et al. Clinical and angiographic outcome in the laserangioplasty for restenotic stents (LARS) multicenter registry. Catheterizationand Cardiovascular Interventions: Official Journal of the Society for CardiacAngiography &Interventions. 2001;52:24-34.
[40]Bilodeau L, Fretz EB, Taeymans Y, Koolen J, Taylor K, Hilton DJ. Novel use of ahighenergy excimer laser catheter for calcified and complex coronary arterylesions. Catheterization and Cardiovascular Interventions: Official Journal ofthe Society for Cardiac Angiography & Interventions. 2004;62:155-61.
[41] DorrM, Vogelgesang D, Hummel A, et al. Excimer laser thrombus elimination for preventionof distal embolization and no-reflow in patients with acute ST elevation myocardialinfarction: results from the randomized LaserAMI study. Int J Cardiol. 2007;116:20-6.
[42] Lee T,Shlofmitz RA, Song L, et al. The effectiveness of excimer laser angioplasty to treatcoronary in-stent restenosis with peri-stent calcium as assessed by opticalcoherence tomography. EuroIntervention: Journal of EuroPCR in CollaborationWith the Working Group on Interventional Cardiology of the European Society ofCardiology. 2019;15:e279-88.
[43]Fernandez JP, Hobson AR, McKenzie D, et al. Beyond the balloon: excimercoronary laser atherectomy used alone or in combination with rotationalatherectomy in the treatment of chronic total occlusions, non-crossable andnon-expansible coronary lesions. EuroIntervention: Journal of EuroPCR inCollaboration With the Working Group on Interventional Cardiology of theEuropean Society of Cardiology. 2013;9:243-50.
[44] HolmesJr DR, Forrester JS, Litvack F, et al. Chronic total obstruction and short-termoutcome: the Excimer Laser Coronary Angioplasty Registry experience. Mayo Clin Proc.1993;68:5-10.
[45] Topaz O,Ebersole D, Das T, et al. Excimer laser angioplasty in acute myocardialinfarction (the CARMEL multicenter trial). Am J Cardiol. 2004;93:694-701.
[46]Bilodeau J. Jean Bilodeau: pioneer in home respiratory care. Interview bySuzanne Blanchet. Infirm Que. 1995;2:24-6.
[47] DahmJB, Topaz O, Woenckhaus C, et al. Laser-facilitated thrombectomy: a newtherapeutic option for treatment of thrombus-laden coronary lesions.Catheterization and Cardiovascular Interventions: Official Journal of theSociety for Cardiac Angiography & Interventions. 2002;56:365-72.
[48] TopazO, Minisi AJ, Morris C, Mohanty PK, Carr Jr ME. Photoacoustic fibrinolysis: pulsed-wave,mid-infrared laser-clot interaction. J Thromb Thrombolysis. 1996;3:209-14.
[49] TopazO, Bernardo NL, Shah R, et al. Effectiveness of excimer laser coronaryangioplasty in acute myocardial infarction or in unstable angina pectoris. Am JCardiol. 2001;87:849-55.
[50] BittlJA, Sanborn TA, Yardley DE, et al. Predictors of outcome of percutaneous excimerlaser coronary angioplasty of saphenous vein bypass graft lesions. The PercutaneousExcimer Laser Coronary Angioplasty Registry. Am J Cardiol. 1994;74:144-8.
[51] WebbJG, Carere RG, Virmani R, et al. Retrieval and analysis of particulate debrisafter saphenous vein graft intervention. J Am Coll Cardiol. 1999;34:468-75.
[52] BaimDS, Wahr D, George B, et al. Randomized trial of a distal embolic protectiondevice during percutaneous intervention of saphenous vein aorto-coronary bypassgrafts. Circulation. 2002;105:1285-90.
[53]Niccoli G, Belloni F, Cosentino N, et al. Case-control registry of excimerlaser coronary angioplasty versus distal protection devices in patients withacute coronary syndromes due to saphenous vein graft disease. Am J Cardiol.2013;112:1586-91.
[54]Giugliano GR, Falcone MW, Mego D, et al. A prospective multicenter registry oflaser therapy for degenerated saphenous vein graft stenosis: the COronary graftResults following Atherectomy with Laser (CORAL) trial. Cardiovasc Revasc Med.2012;13:84-9.
[55]Ebersole D, Dahm JB, Das T, et al. Excimer laser revascularization of saphenousvein grafts in acute myocardial infarction. J Invasive Cardiol. 2004;16:177-80.
作者简介
韩 伟
首都医科大学附属北京安贞医院老年心内科VIP病房 主治医师
中国医科大学临床医学心血管病专业、医学博士
中国科学院动物研究所生物膜国家重点实验室 博士后
中国老年保健协会心血管疾病预防与康复专业委员会 委员
专家简介

刘巍教授
首都医科大学附属北京安贞医院心内科主任医师,副教授,硕士生导师,博士,先后在新加坡国立大学Tan Tock Seng医院,日本东邦大学大森医院心血管介入中心,美国休斯顿德州医学中心Methodist医院Debacky心血管中心及德州大学医学部接受心内科及心血管介入培训
擅长冠心病诊治,结构性心脏介入治疗
目前担任欧洲心脏病学会委员,美国心脏协会委员,中华医学会心血管分会冠心病与动脉粥样硬化学组委员,北京医学会心血管分会青委会副主任委员,中国医师协会心血管分会青年委员